
Robotic & Minimally Invasive Surgery
Performed by Dr. David Wetherell
Robotic and minimally invasive urological surgery allows Dr. David Wetherell to offer precision treatment for a range of prostate, kidney and ureter conditions. Using advanced keyhole techniques, these procedures are designed to minimise discomfort, reduce recovery time and improve patient outcomes.
Robotic Simple Prostatectomy
•
Robotic or Laparoscopic Nephrectomy
•
Robotic or Laparoscopic Partial Nephrectomy
•
Robotic or Laparoscopic Nephro-Ureterectomy
•
Robotic or Laparoscopic Pyeloplasty
•
Retzius-Sparing Robotic Radical Prostatectomy
Robotic Simple Prostatectomy • Robotic or Laparoscopic Nephrectomy • Robotic or Laparoscopic Partial Nephrectomy • Robotic or Laparoscopic Nephro-Ureterectomy • Robotic or Laparoscopic Pyeloplasty • Retzius-Sparing Robotic Radical Prostatectomy
Robotic Simple Prostatectomy
The Key Things to Know:
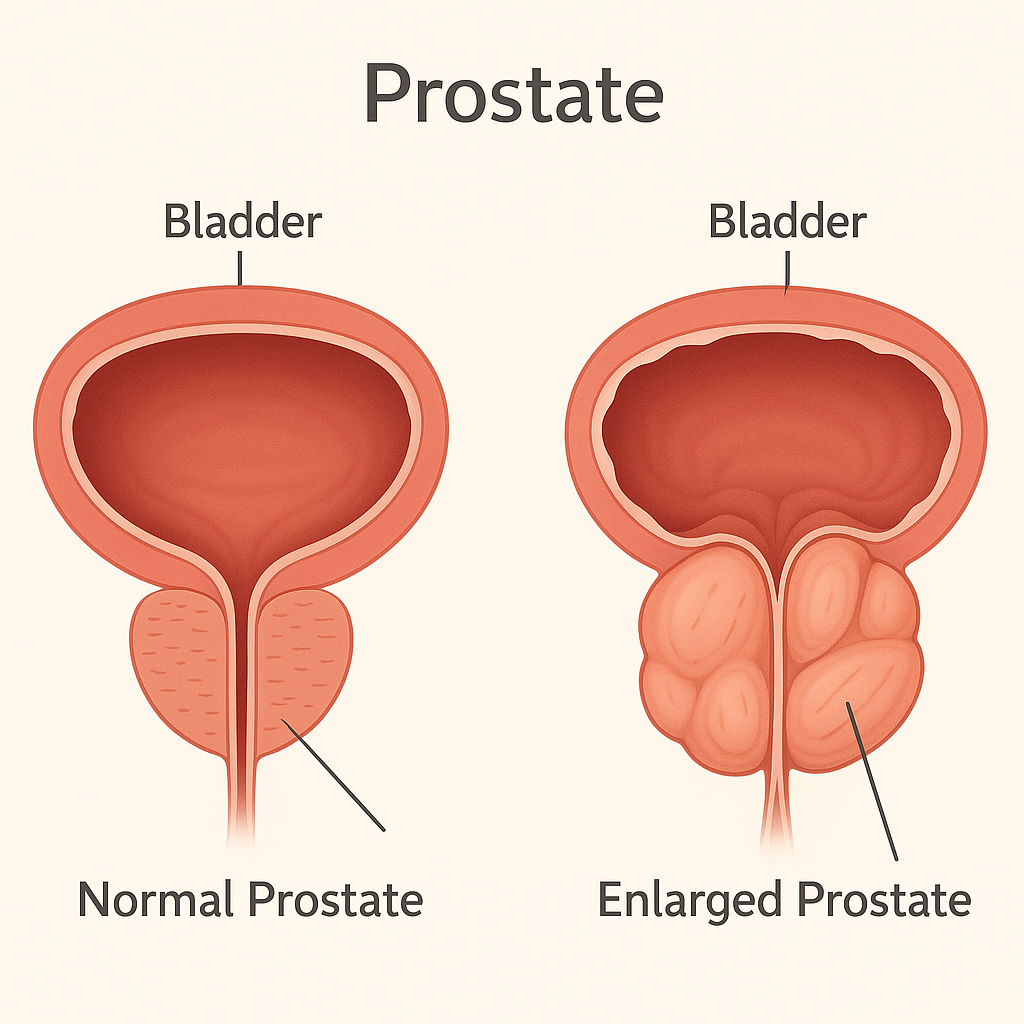
A simple prostatectomy is a surgical procedure to remove the enlarged inner portion of the prostate gland, causing urinary blockage from benign prostatic hyperplasia (BPH). It is generally reserved for very large prostates (usually >150–200g) and provides long-term symptom relief.
What It Is
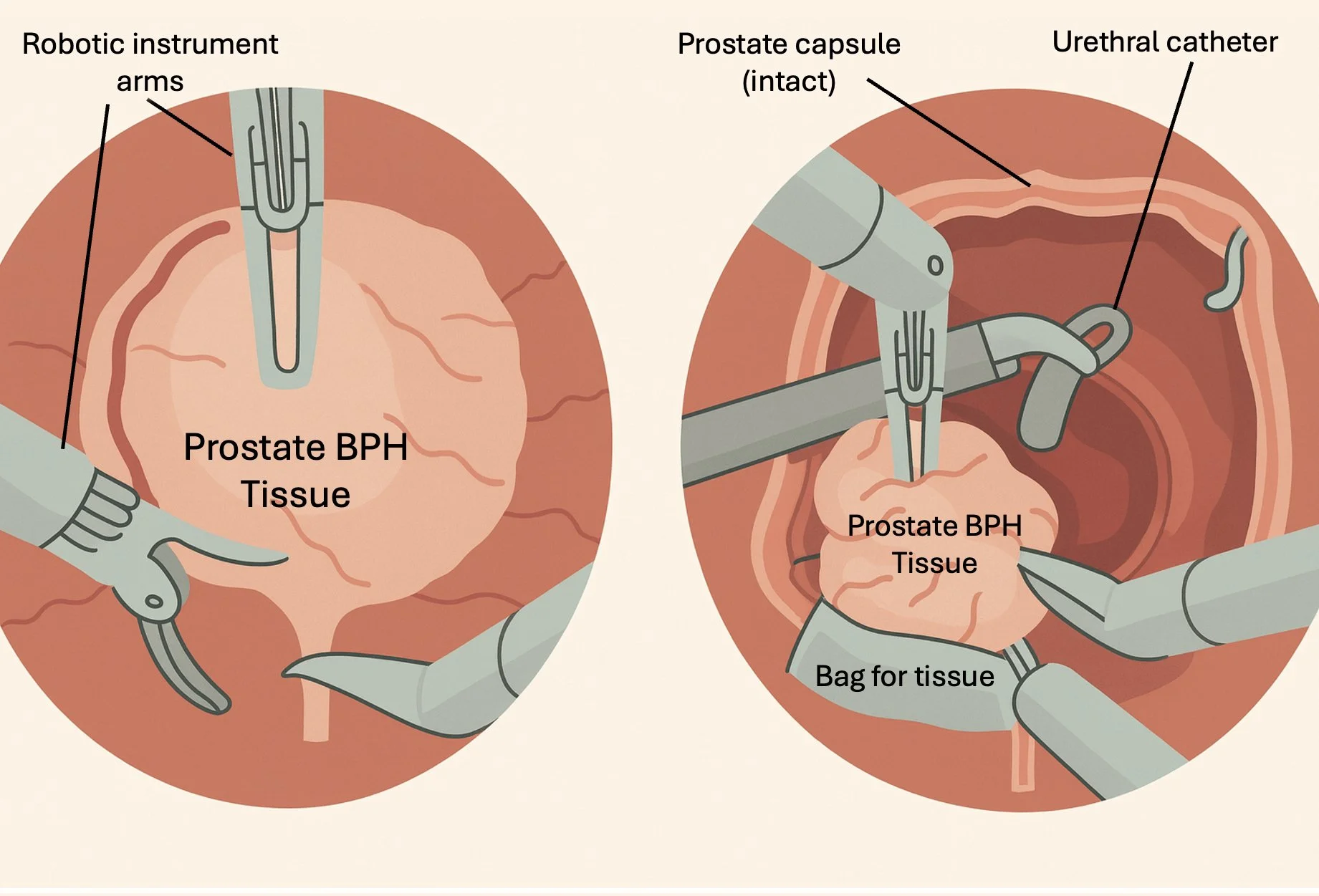
Unlike radical prostatectomy for cancer, a simple prostatectomy removes only the obstructing inner tissue. It can be performed through robotic or in select cases open surgery. The surgeon shells out the adenoma (enlarged tissue) to create a wide open channel for urine flow.
When It's Needed
This operation is recommended for men with very large prostates where TURP or laser surgery would be less efficient, or if there are associated bladder stones or diverticula. It is also considered when patients have chronic retention or kidney effects from obstruction.
Surgery Diagram
Benefits
Excellent long-term symptom relief
Suitable for very large prostates
Low recurrence rates
Can address associated bladder stones or diverticula at the same time
Risks
Bleeding and need for transfusion (higher
than endoscopic surgery)Temporary catheter for several days
Infection or urinary tract infection
Retrograde ejaculation (common)
Rarely, stress incontinence or urethral stricture
What to Expect After Surgery
You will usually stay in hospital for 2–3 days. A catheter remains in place until healing occurs. Mild discomfort and blood in the urine are normal for a few days. Full recovery takes several weeks. Urinary symptoms typically improve dramatically, and recurrence is rare.
FAQs
-
Yes – this surgery is for benign enlargement, not cancer, and the outer capsule of the prostate is left in place.
-
Usually 3–5 days, depending on healing and urine flow.
-
Yes – robotic can reduce bleeding and shorten hospital stay.
Robotic or Laparoscopic Nephrectomy
The Key Things to Know:
A robotic or laparoscopic nephrectomy is a minimally invasive operation to remove all or part of a kidney through small incisions using advanced camera and instrument technology. It is performed to treat kidney cancer, large benign tumours, or a severely damaged non-functioning kidney.

What It Is
During the procedure, several small incisions (usually 5–10 mm) are made in the abdomen. The surgeon uses a high-definition camera and fine robotic or laparoscopic instruments to carefully dissect and remove the kidney. The specimen is removed through a small extraction site.
The robotic approach allows greater precision, stability, and 3D vision, which can improve outcomes compared with standard laparoscopy.
When It's Needed
Nephrectomy may be recommended for:
Localised kidney cancer (most common reason)
A non-functioning or severely scarred kidney
Large benign tumours or cysts
Severe kidney damage from obstruction or infection
Surgery Diagram
Benefits
Minimally invasive – smaller incisions, less pain
Shorter hospital stay (typically 1–3 days)
Faster recovery compared to open surgery
Low complication and transfusion rates (<5%)
Excellent cancer control for localised tumours
Risks
Bleeding (≈2–4%)
Infection or wound complications (≈3–5%)
Injury to nearby organs or bowel (rare, <1%)
Hernia at incision site (≈1–2%)
For radical nephrectomy – loss of kidney function (remaining kidney usually compensates)
What to Expect After Surgery
Most patients stay in hospital for 1–3 days. A urinary catheter and sometimes a drain are used briefly. You can expect mild discomfort around the incision sites and some fatigue for a week or two. Walking and light activities are encouraged early. Avoid heavy lifting for 4–6 weeks.
FAQs
-
Usually not – the remaining kidney typically maintains normal function.
-
Most patients return to normal daily activity within 2–3 weeks and full recovery within 4–6 weeks.
-
Both are safe and effective; the robotic approach offers greater precision and vision, which may reduce blood loss and speed recovery.
Robotic or Laparoscopic Partial Nephrectomy
The Key Things to Know:
A robotic or laparoscopic partial nephrectomy is a minimally invasive operation to remove a kidney tumour while preserving the healthy portion of the kidney. It offers excellent cancer control for small kidney tumours (usually <4 cm) while maintaining kidney function.
What It Is
Under general anaesthetic, the surgeon uses robotic or laparoscopic instruments through several small incisions. The affected part of the kidney containing the tumour is carefully dissected and removed, while the rest of the kidney is preserved. The robotic system provides 3D vision and precise control for delicate suturing to reconstruct the kidney after tumour removal.
When It's Needed
Partial nephrectomy is recommended when:
The kidney tumour is small (usually <4 cm, but up to 7 cm in selected cases)
The tumour is localised and confined to the kidney
Both kidneys are functioning and kidney preservation is desirable
There is a solitary kidney or pre-existing kidney impairment
Surgery Diagram
Benefits
Equivalent cancer control to full nephrectomy for small tumours
Preserves kidney function and reduces long-term risk of kidney failure
Minimally invasive with smaller incisions, less pain, and faster recovery
Hospital stay typically 1–3 days
Risks
Bleeding (≈3–5%)
Urine leak from repair site (≈3–8%)
Infection or wound complications (≈3–5%)
Temporary reduction in kidney function
Rare conversion to full nephrectomy (<2%)
What to Expect After Surgery
Most patients stay 1–3 days in hospital. A urinary catheter and drain are used for 1–2 days. Mild flank discomfort and fatigue are normal. You’ll be encouraged to walk early and gradually return to daily activity over 2–3 weeks. Avoid heavy lifting for 4–6 weeks. Follow-up scans are arranged to check healing and monitor for recurrence.
FAQs
-
Yes – the goal of partial nephrectomy is to remove only the tumour and preserve as much normal kidney as possible.
-
Robotic-assisted surgery allows greater precision and may reduce bleeding and complications compared to standard laparoscopy.
-
Cancer control rates exceed 95% for small, localised tumours.
Robotic Or Laparoscopic Nephro-Ureterectomy
The Key Things to Know:
A robotic or laparoscopic nephro-ureterectomy is a minimally invasive operation to remove the kidney and entire ureter (the tube carrying urine to the bladder). It is performed mainly to treat upper urinary tract urothelial carcinoma (UTUC) - a type of cancer arising in the lining of the kidney or ureter.
What It Is
Under general anaesthetic, several small incisions (5–10 mm) are made in the abdomen. The surgeon uses fine robotic or laparoscopic instruments to remove the kidney, the entire ureter, and a small cuff of bladder around where the ureter enters. The robotic system provides 3D vision and enhanced precision. The specimen is removed through a small incision.
When It's Needed
This procedure is recommended for:
Upper urinary tract urothelial carcinoma (UTUC)
Recurrent ureteric tumours after previous endoscopic management
High-grade or invasive disease requiring complete removal of the affected kidney and ureter
Surgery Diagram
Benefits
Minimally invasive – smaller incisions, less pain
Shorter hospital stay (typically 2–4 days)
Equivalent cancer control to open surgery
Faster recovery and reduced blood loss
Risks
Bleeding requiring transfusion (≈3–5%)
Infection (≈5–10%)
Urine leak or delayed healing at bladder cuff site (≈3%)
Injury to nearby organs or bowel (rare, <1%)
Recurrence of urothelial cancer in the bladder (≈20–30%)
What to Expect After Surgery
You’ll stay in the hospital for about 2–4 days. A catheter and drain are used temporarily. Mild abdominal discomfort, fatigue, and bloating are common early on. Gradual mobilisation is encouraged. You’ll usually return to light activity in 2–3 weeks and full recovery by 4–6 weeks. Follow-up cystoscopies and imaging are essential to monitor for recurrence.
FAQs
-
Because UTUC often spreads to the area where the ureter joins the bladder, removing a small cuff reduces recurrence risk.
-
Yes – the remaining kidney typically compensates and maintains adequate function.
-
Yes – 20–30% may develop new bladder tumours, which are usually managed with surveillance and early treatment.
Robotic Or Laparoscopic Pyeloplasty
The Key Things to Know:
A robotic or laparoscopic pyeloplasty is a minimally invasive procedure used to repair a narrowing or blockage where the kidney joins the ureter (the uretero-pelvic junction, or UPJ). This operation restores normal urine drainage and protects kidney function. Success rates are high, typically over 90%.
What It Is
Under general anaesthetic, several small incisions (5–10 mm) are made in the abdomen. Using a laparoscope or robotic instruments, the surgeon removes the narrowed segment and re-joins the healthy ends of the ureter and kidney (a procedure called anastomosis). A temporary stent is placed to support healing and is removed a few weeks later.
When It's Needed
Pyeloplasty is recommended when:
UPJ obstruction causes pain, infection, or hydronephrosis (swelling of the kidney)
Imaging shows reduced drainage or function of the affected kidney
Stones or crossing vessels contribute to obstruction
Surgery Diagram
Benefits
Minimally invasive – small incisions, less pain
Excellent long-term success (>90%)
Short hospital stay (1–2 days)
Preservation of kidney function
Risks
Urine leak at the repair site (≈2–5%)
Infection or fever (≈5%)
Bleeding requiring transfusion (≈2%)
Stricture recurrence requiring re-intervention (≈5–10%)
Rare injury to nearby organs (<1%)
What to Expect After Surgery
You’ll stay in the hospital for 1–2 days. A urinary catheter and small drain may be placed for 24–48 hours. The internal stent is typically removed 4–6 weeks later via a short cystoscopy. Most patients return to normal activity within 2–3 weeks and full recovery by 4–6 weeks.
FAQs
-
More than 90% of patients have long-term relief of obstruction and pain.
-
Yes – a temporary stent is left in the ureter to support healing and is removed later in clinic.
-
Both robotic and laparoscopic pyeloplasty are effective; robotic surgery offers greater precision and dexterity, especially in complex cases.
Etzius-Sparing Robotic Radical Prostatectomy
Introduction:
Retzius-Sparing Robotic Radical Prostatectomy (RS-RARP) is an advanced keyhole (robotic) technique for treating prostate cancer. It removes the prostate through the space behind the bladder, helping to preserve the structures that control urinary continence and support faster recovery of bladder control.
What It Is
This technique removes the prostate while avoiding disruption of the front of the bladder (the Retzius space). By working behind the prostate, the surgeon preserves key structures that are vital for bladder control and sexual function, including:
The bladder-neck support structures
The urinary sphincter complex
The pelvic floor and neurovascular bundles
The operation is performed through several small incisions in the lower abdomen. The da Vinci® robotic system provides 3D-magnified vision and precise, tremor-free control, allowing delicate surgery around these vital structures.
The Key Things To Know
Minimally invasive keyhole robotic surgery using the da Vinci® system
Performed through the space behind the bladder (Retzius-sparing)
Faster recovery of urinary control – around 80–90% pad-free by 3–6 months
Similar cancer control to standard robotic prostatectomy
Often just one night in hospital with rapid return to activity
When It’s Needed
RS-RARP is usually recommended for men with localised prostate cancer (disease confined to the prostate). It may be suitable if you have:
Low to intermediate-risk prostate cancer suitable for surgery
A prostate of appropriate size and shape for keyhole surgery
Good general health to undergo anaesthesia
It may not be suitable for men with very large prostates, extensive previous pelvic surgery, or cancer extending outside the gland.
Surgery Diagram
Benefits
Faster return of urinary control – 70–90% pad-free at 3 months
Earlier recovery of erections in selected men where nerve-sparing is possible
Equal or lower rates of positive surgical margins
Less disruption to bladder support and pelvic anatomy
Shorter hospital stay and faster overall recovery
Risks
All surgery carries some risks, although serious complications are uncommon. Your surgeon will discuss these with you in detail.
Common temporary effects:
Mild bleeding or infection (around 1–2%)
Short-term urinary leakage (improves with time)
Fatigue for 1–2 weeks
Less Common Risks
Erectile dysfunction (depends on nerve preservation)
Hernia or fluid collection (< 1%)
Positive cancer margin (≈ 10–20%)
What to Expect After Surgery
Hospital stay: Usually 1 night
Catheter: Kept in place for around 5–7 days
Pain: Generally mild and managed with tablets
Driving or light work: Often after 1–2 weeks
Return to sport or heavy activity: After 4–6 weeks
Follow-up: PSA blood test at around 6 weeks post-op
Continence: Most men regain good control within 6–12 weeks
Erections: May take 6–18 months to recover – treatments are available to help
FAQs
-
Not always, it depends on your anatomy, cancer stage, and prior surgery.
-
Yes. It has comparable cancer outcomes with faster recovery of bladder control.
-
Usually 2–3 hours under general anaesthesia.
-
Most men resume normal daily activity within 2 weeks and exercise after 4–6 weeks.
-
Further treatment such as radiotherapy can still be offered safely if required.
Discover Expert Urological Care
I specialise in precision urology using the latest robotic and minimally invasive techniques. Explore my approach, my procedures, and the care I provide at every stage of your journey.

About Dr. David Wetherell

